Hi everyone- hope you are all having a productive week!
De-escalation is such an important tool to have in our clinical practice.
How many of us have faced an angry patient or family member? The public’s stress levels are high, and coupled with our staffing shortages and long waiting times, it seems like a recipe for unpleasant, sometimes out-of-control confrontations.
As a manager, I have learned from experience that being able to de-escalate a situation results in both the healthcare practitioner and the patient/family member leaving happier at the end of the encounter. This means no escalation to management and written complaints that get you called into an office to explain what occurred. It is important to resolve situations as they arise.
Are we as healthcare practitioners confident in our ability to de-escalate a situation? De-escalation isn’t about “winning an argument” or “proving you’re right.” It’s about regulating emotion to restore safety and communication. Here is a comprehensive, actionable toolkit you can use in your everyday clinical practice
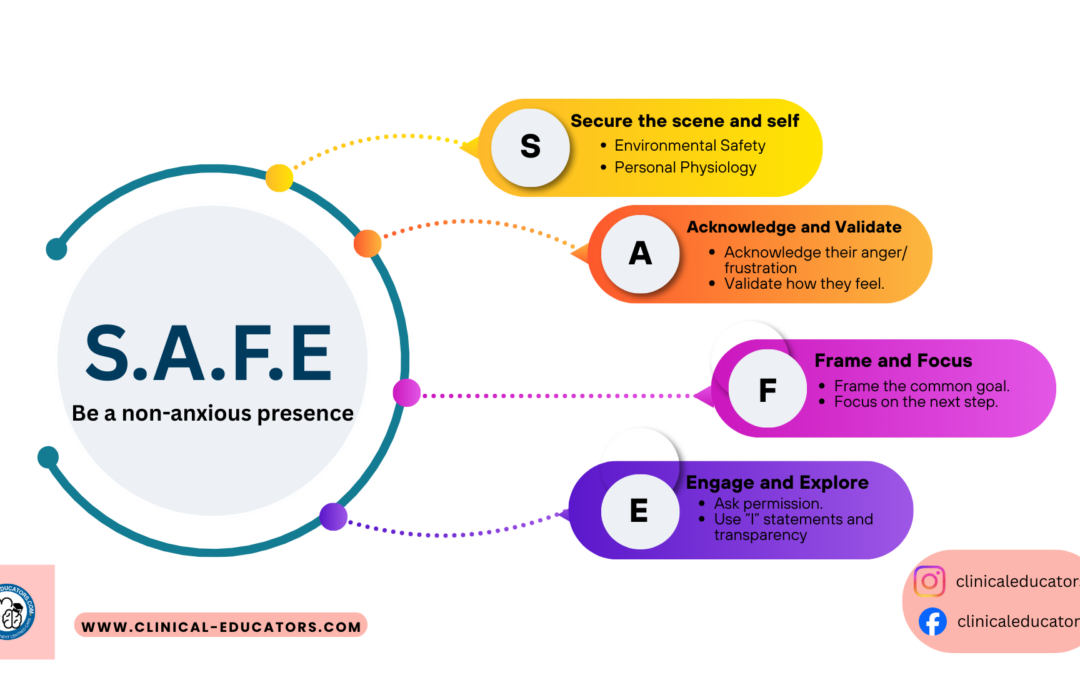
The S.A.F.E. Dialogue Framework for De-escalation.
This is a handy framework to download and display in your work area so all staff are aware of what steps to take if faced with a situation where they need to de-escalate.
STEP 1: S – SECURE the SCENE & SELF (0-30 seconds)
Before you engage with words, manage safety and your own physiology.
1. Environmental Safety:
- Positioning: Stand at an angle, not square-on (confrontational). Keep an open posture. Maintain a safe distance (1.5-2 arm lengths).
- Escape Route: Never let them block you from the door. Position yourself between them and the exit.
- Remove Audiences: “Let’s step into this quiet room so we can talk privately.” This removes performance pressure.
2. Personal Physiology (The 90-Second Rule):
- When faced with aggression, your amygdala hijacks your brain for 90 seconds. Your first job is to manage YOUR reaction.
- Internal Script: “This is not about me. This is fear/pain/grief speaking.”
Micro-Actions: Drop your shoulders. Unclench your jaw. Breathe slowly into your belly. Your calm is contagious.
STEP 2: A – ACKNOWLEDGE & VALIDATE
You must verbally “catch” their emotion before you can address their concern. This is the most crucial step.
The Wrong Response: “Calm down.” “It’s policy.” “You’re misunderstanding.”
The Right Response: Name the emotion and justify it.
Their Emotion Validating Script
- Anger/Yelling: “You’re rightfully furious. This shouldn’t have happened.” “I hear the frustration in your voice, and it’s completely understandable.”
- Fear/Anxiety: “This is terrifying. Anyone in your shoes would be scared.” “You’re carrying a huge weight of worry. That makes so much sense.”
- Grief/Despair: “This is unbearably sad. There are no words.” “Your world has been shattered. Nothing about this is fair.”
- Impatience: “You’ve been waiting forever. You should have been seen by now.”
Why this works: Validation tells the limbic system (emotional brain), “You are heard. You can stop screaming.” It creates psychological safety. The moment they feel truly heard, the emotional charge drops by 50%.
STEP 3: F – FRAME & FOCUS
Once emotion lowers, redirect energy toward a shared goal.
1. Frame the Common Goal: Use “WE” language.
- “We both want the same thing: for your mother to be safe and comfortable.”
- “Let’s figure this out together. You’re the expert on your wife; I’m the expert on the medicine. We need both.”
2. Focus on the Next Step (Not the Whole Mountain):
- Don’t say: “We need to talk about the full treatment plan.”
- Do say: “The most important thing right now is to manage her pain. Can we focus on that first step together?”
- Offer micro-choices to restore their sense of control: “Would it help if I explained the process first, or would you prefer to see her right now?”
STEP 4: E – ENGAGE & EXPLORE
Now, and only now, can you address the actual issue.
1. Ask Permission: “Would it be okay if I shared what I know about the situation?” (This is powerfully disarming).
2. Use “I” Statements & Transparency:
- “I need to be transparent with you. I don’t know why the scan is delayed, but I will find out and bring that answer to you in 15 minutes.”
- “I can’t change the visiting policy, but I can make sure you get a phone update every two hours.”
3. Explore Their Request: Often, the stated demand (“I want to see the CEO!”) masks a core need (feeling powerless, needing reassurance).
- “Help me understand, what would getting an apology from the doctor do for you?” (Might reveal: “I need to know it won’t happen again to someone else.”) You can now address the need.
The Non Negotiables & Danger Sign
What NEVER to do:
- Never argue or correct facts in the emotional phase. (“Actually, it’s been 58 minutes, not an hour…”)
- Never make promises you can’t keep. (“The doctor will be right out.”)
- Never touch without permission (can be perceived as a threat).
- Never take the anger personally (the “It’s not about me” mantra).
DANGER SIGNS Requiring Security:
- Closed fists, pacing, punching walls.
- Invasive proximity (getting in your face).
- Racist, sexist, or personally violent threats.
Your Script: “I want to help you, but for both of our safety, I need to take a step back. I am going to get [the charge nurse/security] so we can all talk safely.” Then disengage and get help.
The Neuroscience Behind It: The “Name It to Tame It” Principle
When you accurately label someone’s emotion (“You’re terrified”), you activate their prefrontal cortex (the rational brain) and dampen the amygdala (the fear/anger centre). Validation isn’t “being nice”—it’s a neurological intervention.
Here is a summarised framework you can keep handy for when you need it:
https://drive.google.com/file/d/1GYB2CFQND0OSvd6n37Vm-QZQzOf4V6ic/view?usp=drive_link
Let me know in the comments what de-escalation methods work for you, and if you find the SAFE framework useful in your clinical practice
Thank you